Blog
How to fix an underbite
How to fix an underbite
What is an Underbite?
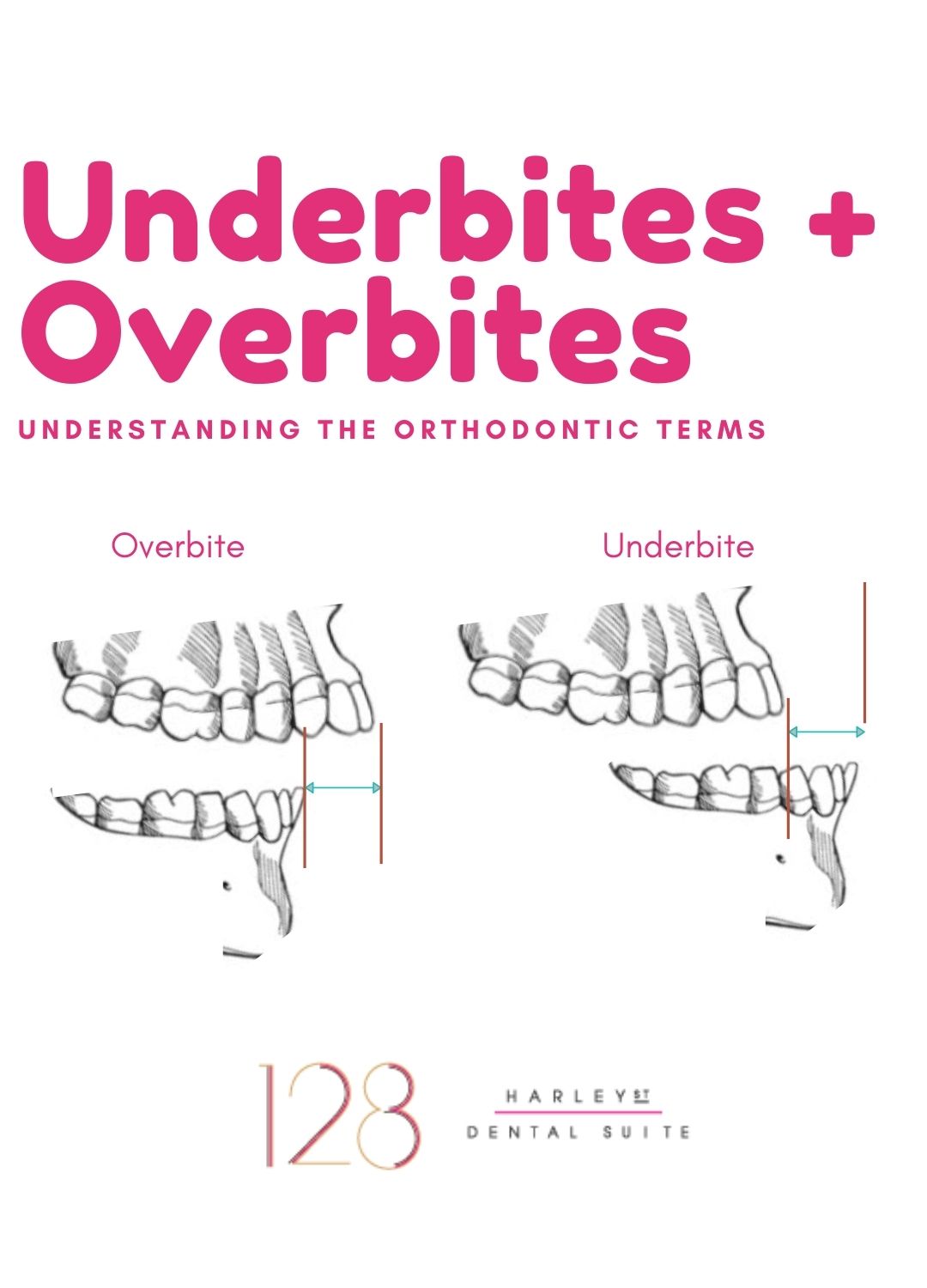
An underbite, first of all, also known professionally as a Class III type of bite, is when the lower teeth extend beyond the upper and ideally the reverse is true, where the top teeth meet the lower teeth by overlapping them. In this type of bite, the lower jaw protrudes beyond the top jaw, making it impossible for the lower row of teeth to align behind the upper row of teeth as they should.
What causes underbites and overbites?
They can be caused by the upper jaw bone being underdeveloped or the bone in the lower jaw being overdeveloped or a combination of both. It can also be due to the position of the teeth, due to a postural habit when closing or due to habits.
Underbites can also result from behaviours like thumb-sucking or caused by genetics or as the result of an accident. Whatever the cause, severe underbites should be treated immediately or as early as possible however there are occasions where delaying treatment is beneficial for you.
Underbites can affect 5-10% of the population and should not be confused with underbites.
Underbites vs Overbites – What are the Differences?
It is once again normal for your top teeth to overlap the bottom teeth and just because your upper teeth extend somewhat over your lower teeth, it doesn’t necessarily mean that you have an overbite. It is also normal for the top teeth to protrude over the lower by a certain degree. It is when this overlap is excessive that you might say that you have an underbite.
Minor overbites are very common and usually no treatment is needed.
What causes an overbite?
The overlap should measure up to 4 millimeters. In excess of this, causes such as:
- genetics
- a small lower jaw
- a small chin
- misaligned bites
- thumb sucking
- poorly fitted crowns
- gum disease
- injury
Also, sometimes its just the position of the teeth.
Overbites are technically referred to as Class II bites, there are a range of of devices that help in correcting this type of bite.
Underbite Treatments
A team of specialist dental surgeons, also known as orthodontists will determine the best course of action to treat your misaligned bite.
Your options could include:
Some treatment options for children with underbites include:
- Removable type of braces such as an upper jaw expander, a device that is placed in the upper jaw which can be widened nightly until treatment is complete.
- A reverse-pull face mask, which wraps around the head and attaches to the braces attached on the back upper teeth to pull the upper jaw forward.
- A chin cap, which restricts the growth of the lower jaw.
- Fixed braces to adjust the position of the misaligned teeth.
- Aligners to render a more discreet type of solution
Will I needed teeth extracted for an underbite?
Depending on your type of underbite or the bite you present with, lengthier treatments, with braces can be accomplished with Dental extractions, to relieve the pressure of overcrowding and help the jaw relax into a more natural position.
Surgery to act as an adjunct to fixed braces to modify the position of the top and bottom jaws.
Please contact us on 02079358777 or via email to organise a consultation to discuss your needs. At 128 Harley Street Dental Suite we aim to tailor the treatment to your needs.
Dr. Stefan Abela
BChD, MFDS, RCS Eng, MSc, MORTH RCS Ed, AHEA, FDS Orth RCS Ed
Stefan is a Consultant in Orthodontics at one of the most prestigious London teaching hospitals; Guy’s and St Thomas NHS Foundation Trust.
Stefan is also a specialist in Orthodontics and is registered on the General Dental Council (GDC) specialist list. Stefan qualified as a dental surgeon in 2003 and underwent further training in various specialties including restorative dentistry, paediatric dentistry, oral medicine and complex oral and maxillofacial surgery including the management of facial trauma.
Management of thumbsucking, is a thumb guard needed?

Many parents worry about their babies and/or children thumb sucking, is this a valid concern to have? Are there any problems with a child or baby sucking their thumb? In this blog post we take a look at some of these questions.
Baby keeping thumb in mouth – is this a problem?
There is a natural tendency for very young babies to feel comfort from having something in their mouth, this is why many babies can develop a habit of sucking a thumb or finger, in fact babies have been photographed and scanned doing this in the womb!

As babies begin to develop it, it is a normal developmental stage to begin oral exploration. The mouth is particularly sensitive and when babies put everyday objects in their mouth it allows them to begin to discover the textures and tastes of the world around them.
When babies put objects in their mouth it can also be a sign that the first teeth are beginning to come through.
Is this a problem?
A baby that keeps their thumb in their mouth can be a problem as the constant pressure on the roof of the mouth, which is caused as the baby sucks, can begin to move the bone.
If this habit continues through into early, mid or even late childhood the bone will continue to move with this pressure. It’s a very similar process to orthodontics, orthodontic braces work by applying pressure to the tooth which moves them through the bone, when a baby sucks very hard the pressure is simply applied to the bone directly by their thumb.
This can end result in an anterior open bite where the front teeth don’t meet leading to dental work later on in life.
 If your baby or child consistently sucks their thumb it may be worth considering providing an alternative appliance which allows them to soothe themselves without putting the pressure on the bone.
If your baby or child consistently sucks their thumb it may be worth considering providing an alternative appliance which allows them to soothe themselves without putting the pressure on the bone.
Toddlers fingers in mouth constantly – is this a problem?
This has the same effect as babies putting fingers and thumbs in their mouth, in and of itself it is not a problem however if the pressure on the roof of the mouth is such that the bone moves it can cause orthodontic problems later on in life.
If your toddler has teeth coming through then the pressure of the fingers in their mouth can move the baby teeth. As the baby teeth move the bone will also move which will in turn move the permanent teeth which are yet to come through.
If this habit continues swallowing and speech can also be affected as the bone moves in the oral environment.
How to fix overbite from thumb sucking
Many cases of overbite, including those caused by thumbsucking can be successfully treated using most types of braces including orthodontic fixed appliances (on the outside of the teeth), Invisalign® or other type of clear aligners or braces on the inner aspect of the teeth; also known as lingual braces such as Win GmbH or Incognito™.
If you believe that your child has been sucking their thumb and moving the bone then it is recommended that you visit an orthodontist as early as possible, even as young as 5 years old. Early intervention orthodontics can help to assess the likelihood of problems developing later on in life and then help to prevent them throughout the developmental stages of your child and as they grow.
Management of thumb sucking
It is possible to help a child to stop sucking their thumb with 2 key areas:
- preventive therapy
- appliance therapy
Preventative therapy includes:
- Painting the nails with a bitter or foul tasting liquid
- Wearing a finger guards over the hands including gloves
- Making the child where a thumb sucking guard
- Putting the child into a long sleeved gown so they can’t get access to their thumbs or fingers
- Age appropriate discussions and explanations with the child and positive re-inforcements such as a sticker chart
Appliance therapy includes:
- Fixed appliances to break the habit by making the habit as difficult as possible to continue
- Removeable appliances to break the habit by making the habit as difficult as possible to continue
Reference: Shetty RM, Shetty M, Shetty NS, Deoghare A. Three-Alarm System: Revisited to treat Thumb-sucking Habit. Int J Clin Pediatr Dent 2015;8(1):82-86
Do thumb guards work?

Yes. They can work incredibly well to prevent thumbsucking so long as it is used in conjunction with other techniques. A child could get incredibly frustrated if they are unable to soothe themselves by sucking her thumb. This could lead to creation of other undesirable habits or they could move the habit to fingers which are not covered by the guard.
Positive reinforcement is recommended to ensure that each day or night that the child goes without sucking their thumb is recognised by the parent and that the child feels good about themselves and their achievements. A sticker chart can work really well for this to help the child assess their progress and be rewarded when they stop their finger and thumb sucking.
Should I use a pacifier (dummy) to replace a thumb

It is recommended that children do not have dummies beyond the age of about 4 or 5. if you feel you would like to switch your child over to using a pacifier instead of their thumb then it is recommended that an orthodontic dummy is used.
if a decision is made to replace thumb and finger sucking with a pacifier then it is recommended that an orthodontic pacifier/dummy is used.
These orthodontic dummies are shaped to prevent the excessive forces which are applied to the roof of the mouth during regular thumb sucking. However, they do not completely eliminate these forces so even orthodontic dummies should be used with caution.
Summary
Most orthodontists are agreed that thumbsucking, if it continues in to childhood can indeed cause long-term orthodontic problems for the children as they grow into adults. It is therefore recommended to try and break the thumbsuckers habit as as soon as possible to avoid future problems.
Dr. Stefan Abela
BChD, MFDS, RCS Eng, MSc, MORTH RCS Ed, AHEA, FDS Orth RCS Ed
Stefan is a Consultant in Orthodontics at one of the most prestigious London teaching hospitals; Guy’s and St Thomas NHS Foundation Trust.
Stefan is also a specialist in Orthodontics and is registered on the General Dental Council (GDC) specialist list. Stefan qualified as a dental surgeon in 2003 and underwent further training in various specialties including restorative dentistry, paediatric dentistry, oral medicine and complex oral and maxillofacial surgery including the management of facial trauma.